Before treating acne scars, it is essential to thoroughly treat active acne first.
This is because acne is the root cause of scarring, including pitted scars and redness. Without addressing the underlying cause, new scars will continue to form.
In some cases, patients may have subtle acne lesions that they are unaware of, causing chronic inflammation in the skin.
During consultation, if active acne is present, our clinic will recommend comprehensive “acne treatment” alongside acne scar therapy.
Acne Treatment
Acne TreatmentComprehensive acne treatment with isotretinoin and hormonal therapy. HADA NO CLINIC Tokyo offers advanced oral medications and personalized treatment plans from experienced dermatologists with 16 years of expertise.
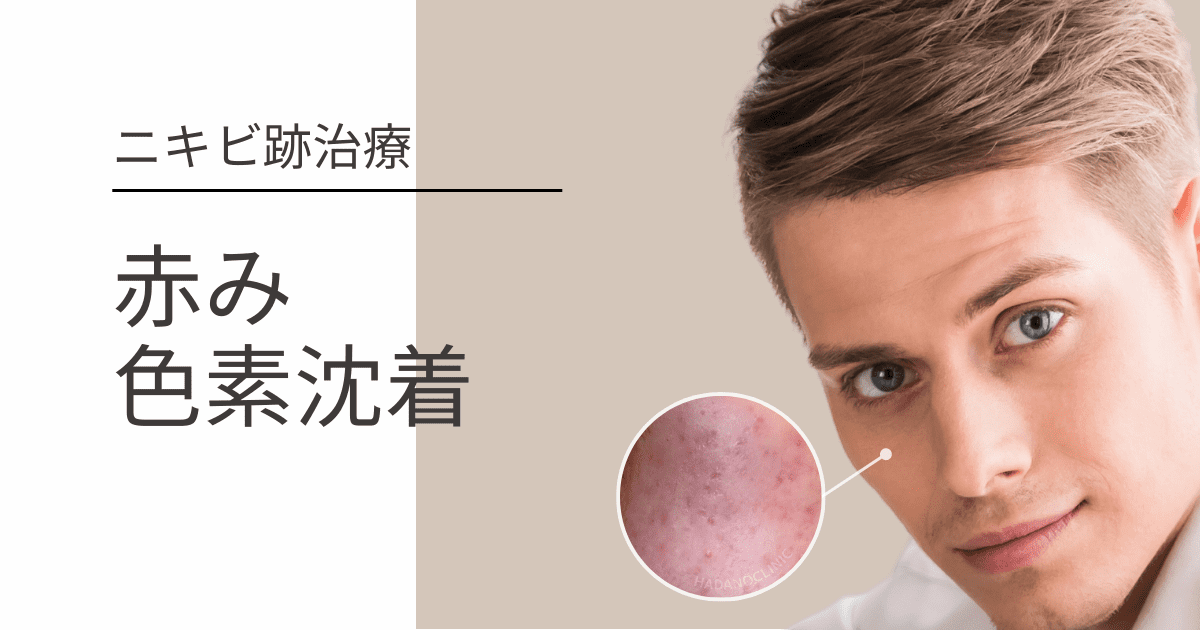
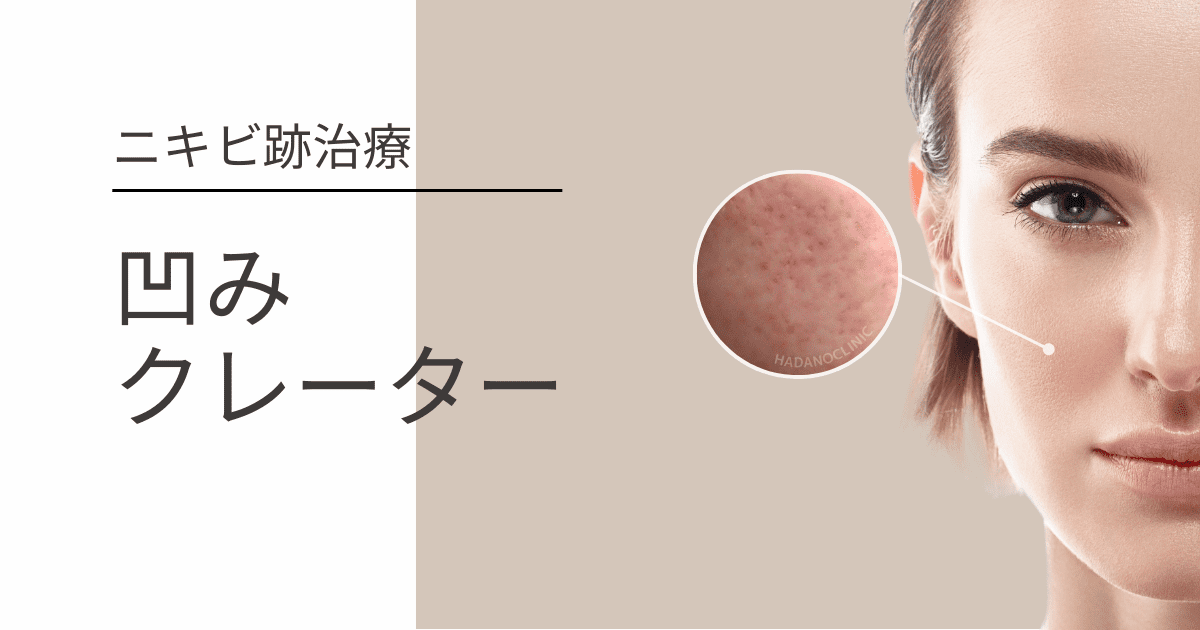
HADA NO CLINIC’s Acne Scar Treatment
Hada no Clinic’s acne scar treatment is categorized into three main types based on scar characteristics. Please refer to each dedicated page for detailed information.